Flabs
Myeloblast vs Lymphoblast: Important Differences
In pathology, bone marrow blast identification guides leukaemia classification and treatment. During smear review or digital morphology analysis, you evaluate immature precursors and assign lineage with precision. Two blast populations dominate acute leukaemia diagnostics: myeloblasts and lymphoblasts.
Pathologists compare nuclear structure, cytoplasmic features, staining, and immunophenotype before reaching a conclusion. Even small variations influence interpretation, especially during early disease stages or ambiguous marrow samples.
In that sense, a clear comparison of myeloblast vs lymphoblast supports faster lineage recognition during microscopic examination.
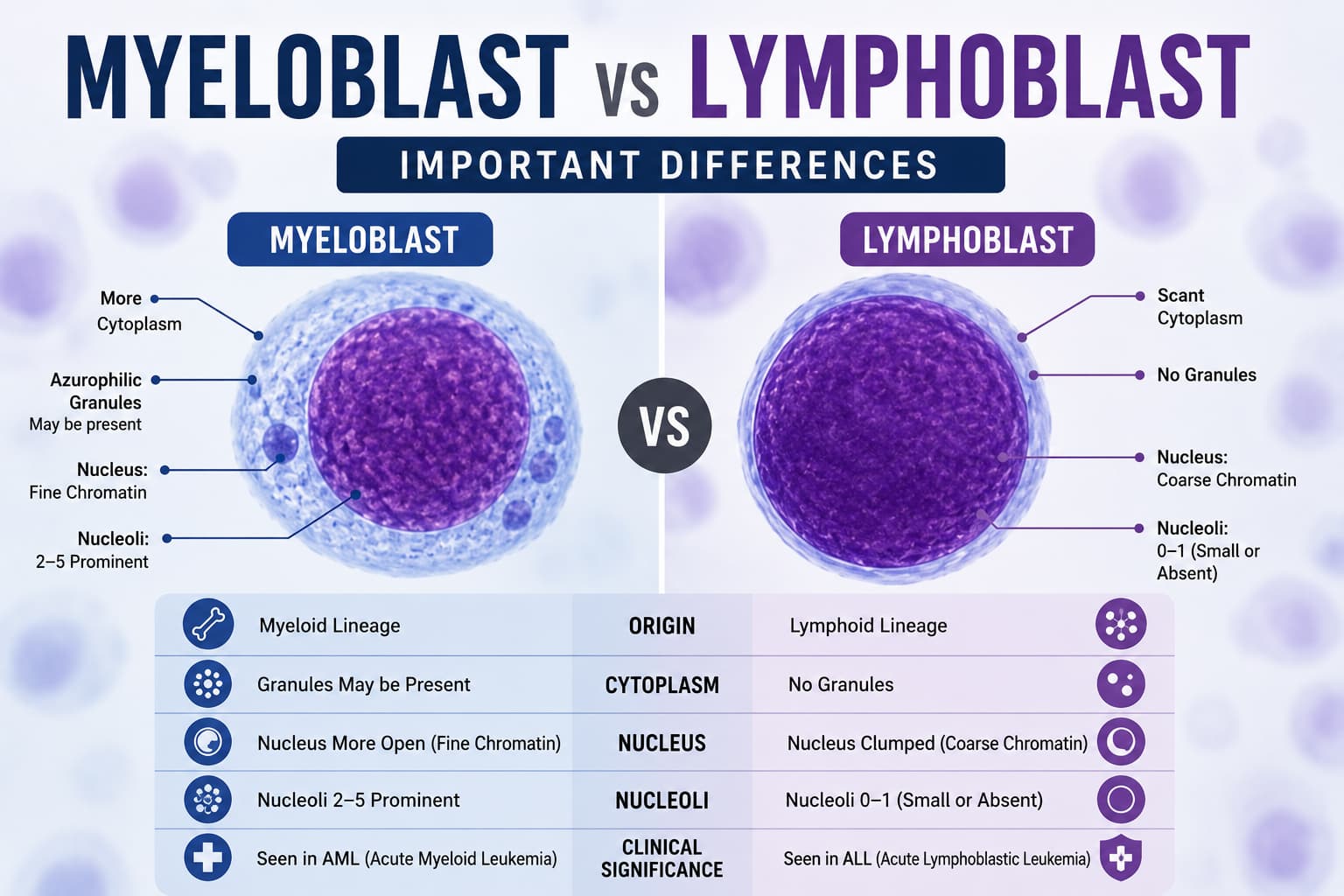
Myeloblast vs Lymphoblast: A Brief Comparison
| Feature | Myeloblast | Lymphoblast |
|---|---|---|
| Definition | Immature white blood cells formed in the bone marrow | Immature precursor cells that mature into lymphocytes |
| Lineage | Myeloid lineage precursor | Lymphoid lineage precursor |
| Differentiates Into | Neutrophils, eosinophils, and basophils | B lymphocytes and T lymphocytes |
| Cell Size | Approximately 15–20 µm | Approximately 10–18 µm |
| Nucleus Shape | Curved or irregular; may appear S-, V-, or C-shaped | Mostly round |
| Nucleus Size | Smaller relative to lymphoblast nucleus | Larger nucleus with dense chromatin pigments |
| Nuclear Chromatin | Fine, delicate meshwork | More condensed or clumped |
| Number of Nucleoli | Usually 2–5 prominent nucleoli | Usually 1–2 nucleoli, less conspicuous |
| Cytoplasm | Scant to moderate, blue staining; may contain granules and Auer rods | Very scant cytoplasm, blue, agranular |
| Cytoplasmic Granules | May be present depending on subtype | Absent |
| Subtypes | Granular, pauci-granular, agranular | No granule-based subtypes |
| Clinical Association | Increased numbers seen in acute myeloid leukemia (AML) | Overproduction associated with acute lymphocytic leukemia (ALL) |
Lymphoblast and Myeloblast in Pathology
Lineage identification begins with blast morphology. A pathologist examines blast size, nucleoli, chromatin pattern, cytoplasm, and granulation. Clear separation in myeloblast vs lymphoblast influences classification in acute leukemias such as AML and ALL.
When you assess myeloblast vs lymphoblast under microscopy, several structural patterns influence interpretation of the test.
- Nuclear chromatin density
- Nucleoli prominence
- Cytoplasmic granules
- Nuclear-cytoplasmic ratio
- Cytoplasmic basophilia
Each observation contributes to lineage assignment. Myeloid blasts derive from granulocytic precursors, while lymphoid blasts originate from B-cell or T-cell progenitors.
Morphologic Characteristics in Blast Examination
Morphology forms the first layer of blast classification. Even before immunophenotyping, smear review reveals lineage clues.
The topic of lymphoblast vs myeloblast morphology appears in haematology training and daily pathology practice. During the review of myeloblast vs lymphoblast review, you will examine several microscopic traits.
Myeloblast Morphology
- Larger cell diameter.
- Moderate cytoplasm with faint basophilia.
- Fine nuclear chromatin.
- Multiple nucleoli.
- Cytoplasmic granules in some cases.
- Possible Auer rods.
The presence of Auer rods immediately points toward myeloid lineage. Granulation intensity varies between cases and disease stages.
Lymphoblast Morphology
- Smaller blast size.
- Very high nuclear-cytoplasmic ratio.
- Deep basophilic cytoplasm.
- Dense chromatin.
- One or two subtle nucleoli.
- No cytoplasmic granules.
Chromatin condensation becomes a distinguishing aspect. During myeloblast vs lymphoblast assessment, chromatin pattern frequently drives the first impression under the microscope.
Cytochemical Staining
Morphology alone may produce uncertainty, particularly in poorly differentiated leukemias. Cytochemical staining introduces another diagnostic layer.
The concept of myeloblast vs lymphoblast stain patterns appears in classical haematology techniques. A decision gains clarity after evaluating stain reactions.
Common cytochemical stains include the following.
- Myeloperoxidase (MPO)
- Sudan Black B
- Periodic acid-Schiff (PAS)
- Nonspecific esterase
Myeloblast Staining Profile
Myeloblast cells show strong positivity with:
- Myeloperoxidase
- Sudan Black B
Both stains identify enzymes within myeloid granules. Positive staining strongly indicates myeloid lineage.
Lymphoblast Staining Profile
- Negative MPO
- Negative Sudan Black B
- PAS block positivity in some lymphoid blasts
During myeloblast vs lymphoblast comparison, MPO positivity carries high diagnostic weight.
Implications in Acute Leukaemia
In the diagnostics of acute leukaemia, blast lineage directs classification and treatment. A precise difference between lymphoblast and myeloblast influences risk stratification, targeted therapy, and decision-making.
In acute leukemia workups, myeloblast vs lymphoblast separation directs lineage assignment within major disease categories.
Acute Myeloid Leukemia (AML): Myeloid blasts dominate marrow and peripheral blood. Myeloblast cells proliferate rapidly and replace normal hematopoiesis.
Acute Lymphoblastic Leukemia (ALL): Lymphoblast proliferation characterizes B-cell or T-cell leukemia variants.
It also guides further testing.
- Flow cytometry immunophenotyping.
- Cytogenetic analysis.
- Molecular mutation panels.
Digital Pathology and Blast Recognition
Digital haematology platforms now support blast detection and classification. Slide scanning and AI-assisted morphology recognition accelerate screening across large smear volumes.
Automated flagging can support myeloblast vs lymphoblast classification during preliminary review. Algorithms analyze nuclear contour, chromatin texture, cytoplasmic area, and staining intensity.
On the other hand, a pathology lab software like Flabs integrates digital microscopy with laboratory information systems (LISs). Such systems allow pathologists to review blast morphology remotely, without physical access. They can even annotate suspicious cells and maintain standardised reporting.
Of course, human expertise still drives final lineage interpretation. Technology simply improves detection speed and reproducibility across laboratories.
Common Challenges
- Poor smear preparation that leads to distorted cell morphology.
- Degenerated blasts in delayed sample processing.
- Hypogranular myeloid blasts lack visible granules.
- Early precursor cells with ambiguous chromatin pattern.
- Therapy-related morphologic changes.
Practical Checklist for Blast Differentiation
- Examine blast size relative to red cells.
- Evaluate chromatin density.
- Identify nucleoli prominence.
- Assess cytoplasmic volume.
- Look for granules or Auer rods.
- Confirm findings with cytochemical stains.
- Correlate with flow cytometry markers.
Conclusion
Blast differentiation is indispensable when it comes to the diagnosis of leukaemia. As discussed, pathologists combine morphology, cytochemical staining, and immunophenotyping to determine lineage.
Consistent assessment of myeloblast vs lymphoblast improves accuracy during bone marrow and peripheral smear review. When you recognise nuclear structure, cytoplasmic features, and stain reactions with precision, lineage classification becomes more reliable.
A strong grasp of the difference between lymphoblast and myeloblast, along with recognition of myeloblast cells in marrow samples, ensures clear distinction during acute leukemia evaluation. Above all, it supports timely diagnosis, targeted therapy, and better proper coordination across haematology teams.
Get Started at ₹1!
Try Flabs for a full month for just ₹1.
Follow us on