Flabs
Cancer Grading and Staging: A Complete Guide
Cancer diagnosis does not end with identifying malignant cells under a microscope. As a pathologist or clinician, you know that it becomes meaningful only after defining how aggressive a tumour appears and how far it has spread.
Two terms dominate that discussion in relation to that: grade and stage.
Is grade and stage the same in cancer? The answer is no.
Each describes a different dimension of disease behaviour. One reflects cellular appearance under microscopy. The other maps the physical spread within the body.
For pathologists, oncologists, and pathology professionals working in modern labs, clarity around these classifications influences treatment, prognosis, and research data.
Cancer Grading and Staging: A Comparison
| Aspect | Cancer Grading | Cancer Staging |
|---|---|---|
| Meaning | Describes how cancer cells look under a microscope and how abnormal they appear. (Cellular appearance) |
Describes how large the tumour is and whether the cancer has spread in the body. (Tumour Spread) |
| Main Idea | Indicates how aggressive the cancer cells are likely to behave. | Indicates how far the cancer has progressed in the body. |
| Memory Tip | Grade = How cells look. | Stage = Size and Spread. |
| Focus | Cell appearance and behaviour. | Tumour size, location, and spread. |
| Determined By | A pathologist examining cancer cells under a microscope. | Doctors use imaging tests, biopsies, and staging systems (like TNM). |
| Purpose | Helps predict the growth speed and aggressiveness of the cancer. | Helps determine the extent of the disease and treatment planning. |
| Scale/Levels | Usually Grade 1–Grade 3. | Usually Stage 0–Stage IV. |
| Low Level | Grade 1: Cells look similar to normal cells and grow slowly. | Stage 0: Abnormal cells present but not spread (carcinoma in situ). |
| Intermediate Level | Grade 2: Cells look somewhat abnormal and grow faster. | Stage 1–2: Cancer present and growing, but with limited spread. |
| High Level | Grade 3: Cells look very abnormal and may grow/spread quickly. | Stage 3–4: Cancer is larger and may spread to lymph nodes or other organs (Stage 4 = metastasis). |
| Clinical Use | Helps predict tumour aggressiveness and recurrence risk. | Helps determine severity, prognosis, and treatment strategy. |
| Change Over Time | May change if tumour characteristics change. | The stage remains the same as the original diagnosis, even if cancer progresses later. |
What is the Difference Between Stage And Grade In Cancer
To start with, cancer grading and staging is the backbone of oncologic classification. When diagnosing cancer, both systems work together to describe tumour behaviour in two complementary ways.
Grade evaluates how abnormal tumour cells look compared with normal tissue.
Stage measures tumour size, lymph-node involvement, and distant spread.
Combine both, and you can gain a structured profile of the severity of the disease.
So, when someone asks, is grade and stage the same in cancer? The answer becomes straightforward:
Grade measures microscopic aggressiveness, while stage measures anatomical spread.
In clinical reports and tumour boards, cancer grading and staging translate pathology findings into a direction for treatment.
- Surgeons assess operability.
- Oncologists select chemotherapy.
- Radiologists correlate imaging findings.
Without clear cancer grading and staging, any discussion around treatment loses its precision.
Why Both Systems Matter in Oncology
A tumour may look aggressive under the microscope. Yet it can remain confined to a small region. Conversely, a low-grade tumour may spread widely before detection.
Consider a scenario.
- A low-grade kidney tumour spreads to distant tissue.
- A high-grade breast tumour remains localised.
Which case demands more aggressive therapy?
Staging answers that question. Grading complements it.
Together, cancer grading and staging deliver a complete clinical picture. Pathologists contribute grading through histopathology, while clinicians combine imaging, surgical findings, and lab reports to determine stage.
Cancer Grades: What Pathologists Evaluate
Grading focuses on cellular morphology. You evaluate differentiation, mitotic rate, and nuclear atypia.
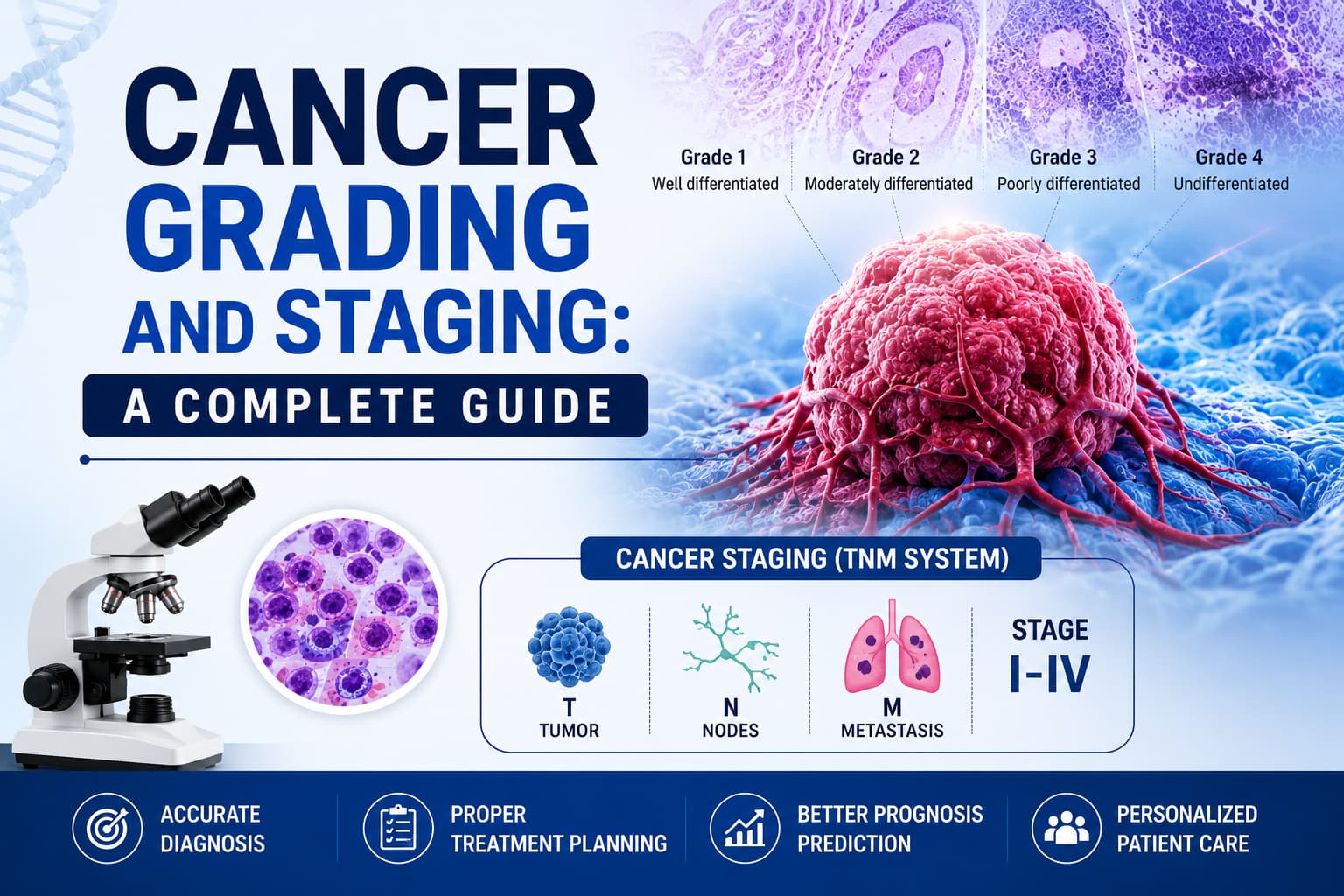
Most tumour grading systems follow four general categories.
| Grade | Cellular Appearance | Behaviour |
|---|---|---|
| Grade 1 | Cells resemble normal tissue | Slow growth |
| Grade 2 | Moderate abnormality | Intermediate growth |
| Grade 3 | Marked abnormality | Rapid growth |
| Grade 4 | Highly undifferentiated cells | Very aggressive |
Pathology reports describing cancer grading and staging frequently include certain grading systems.
- Nottingham grading for breast tumours.
- Gleason grading for prostate tumours.
- Fuhrman or ISUP grading for kidney malignancies.
Cancer Staging: Measuring Tumour Spread
Staging describes the extent of the tumour inside the body. Most systems rely on the TNM classification.
- Tumour (T): Primary tumour size or invasion.
- Node (N): Regional lymph-node involvement.
- Metastasis (M): Distant metastasis.
Within TNM staging, the extent of disease is further defined using a numbering system by organisations such as the National Cancer Institute and MD Anderson Cancer Centre.
Primary tumour (T)
The T category describes the size of the main tumour and how far it has grown into nearby tissues.
- TX: The primary tumour cannot be evaluated or measured.
- T0: No evidence of a primary tumour is detected.
- Tis (tumour in situ): The tumour remains confined to the original tissue layer and has not invaded surrounding tissues; therefore, it cannot metastasise.
- T1 - T4: These categories indicate increasing tumour size or extent of invasion into nearby tissues. A higher number signifies a larger tumour or greater local spread. In some cases, these categories may be further subdivided (for example, T3a or T3b) to provide more specific details.
Regional Lymph Nodes (N)
The N category indicates whether cancer has spread to nearby lymph nodes. Lymph nodes are small, bean-shaped structures that carry lymphatic fluid containing immune cells throughout the body. Because cancer cells often travel through the lymphatic system, nearby lymph nodes are commonly the first location to which cancer spreads.
- NX: The status of nearby lymph nodes cannot be assessed.
- N0: No cancer is found in the regional lymph nodes.
- N1 - N3: These stages represent increasing involvement of lymph nodes. A higher number indicates that more lymph nodes contain cancer or that the affected nodes are located farther from the primary tumour.
Distant Metastasis (M)
The M category identifies whether cancer has spread from the original site to distant organs or tissues in the body.
- MX: The presence of distant metastasis cannot be determined.
- M0: No distant spread of cancer is detected.
- M1: Cancer has spread to distant parts of the body.
Together, the T, N, and M classifications provide a standardised way for healthcare professionals to describe the extent of cancer, which helps guide diagnosis, treatment planning, and prognosis.
Physicians combine these variables into stages ranging from Stage 0 to Stage IV.
A simplified cancer staging and grading chart appears below.
| Stage | Description |
|---|---|
| Stage 0 | Carcinoma in situ |
| Stage I | Localised tumour |
| Stage II | Local growth with limited spread |
| Stage III | Regional lymph-node involvement |
| Stage IV | Distant metastasis |
Role of Pathology Laboratories
Pathology laboratories drive the grading component of cancer grading and staging.
Histopathology sections, immunohistochemistry panels, and molecular assays contribute to detailed tumour characterisation. Many pathology labs in India now integrate digital pathology and AI tools to increase diagnostic consistency. After all, on-time evaluation is imperative in high-volume labs.
Indeed, a modern laboratory relies on several components to ensure precision and speed in outcomes.
- Histopathology instruments and microtomes.
- Automated staining platforms.
- Digital slide scanners.
- Data systems managing lab equipment.
- Reports and case tracking.
Accurate grading begins with reliable specimen processing and high-quality microscopy.
Specific Examples of Cancer Grades and Stages
Every cancer type carries its own grading scale and staging considerations. Let’s review several commonly encountered malignancies.
Breast Tumours
Clinicians frequently discuss breast cancer stages and grades during tumour board meetings. There is a Nottingham grading system that evaluates the following.
- Tubule formation
- Nuclear pleomorphism
- Mitotic activity
Staging depends on tumour size, lymph node spread, and metastases detected by imaging.
Lung Malignancies
For thoracic oncology, stages and grades of lung cancer rely heavily on TNM classification and histological subtype.
Pathologists identify tumour types such as Adenocarcinoma, Squamous cell carcinoma, and Small cell carcinoma.
Small cell carcinoma tends to be more aggressive and to display higher grades. It highlights why cancer grading and staging must be discussed together in clinical settings.
Prostate Tumours
In urologic oncology, prostate cancer staging and grading revolve around the Gleason scoring system.
Gleason patterns describe glandular architecture. Two dominant patterns combine to generate a score ranging from 6 to 10.
A patient with Gleason 6 disease and limited tumour volume receives a very different management plan than someone with Gleason 9 and metastatic spread.
Kidney Malignancies
Renal tumours demonstrate wide variability in behaviour. When reviewing kidney cancer stages and grades, pathologists assess nuclear features, tumour size, and vascular invasion.
High-grade tumours correlate with poorer outcomes, particularly when staging reveals renal vein involvement or distant metastasis.
Again, clinical decisions rely heavily on reliable cancer grading and staging.
Bladder Tumours
Urologists frequently reference bladder cancer stages and grades during cystoscopic surveillance.
Here, two factors dominate the management of the condition.
- Tumour invasion depth
- Histological grade
Non-muscle-invasive tumours may be confined to the mucosa yet recur repeatedly. Pathology reports defining cancer grading and staging determine surveillance frequency and intravesical therapy.
Esophageal Tumours
When evaluating location and grading in oesophageal cancer staging, clinicians assess tumour position along the oesophagus along with histological differentiation.
Upper, middle, and distal segments carry different surgical implications. Grade adds another layer by reflecting tumour aggressiveness.
Again, accurate cancer grading and staging allow surgeons to design tailored resection strategies.
Tests That Support Staging
As mentioned, histopathology guides the grading of cancer tissue. Whereas staging requires integration with imaging and laboratory tests.
The most common imaging tests to accomplish that include the following.
- CT and PET scans.
- MRI imaging.
- Sentinel lymph-node biopsy.
- Tumour markers.
- Blood investigations.
Some clinicians inquire about an ESR test for cancer.
ESR alone does not diagnose malignancy. Elevated ESR may indicate inflammation or systemic disease. Yet physicians sometimes track ESR levels alongside other findings in oncology tests.
Laboratory systems recording such parameters contribute indirectly to the documentation of cancer grading and staging.
Why Accurate Reporting Matters
After diagnosis, major clinical decisions are given in the form of a pathology report. Incomplete pathology reports can slow them and impact outcomes for the patient. Ambiguous grading terms create confusion in tumour boards. Any missing staging data delays therapy also.
Hence, high-quality laboratories focus on structured reporting prescribed by regulated bodies like NABL and ICMR in India. They usually include the following information.
- Histologic tumour type.
- Differentiation grade.
- Margins and invasion.
- Lymph-node status.
- Metastatic findings.
In medical reporting, the importance of structured templates can't be overemphasised. They ensure consistency across departments and improve clarity in cancer grading and staging.
Digital Systems for Reporting
Since manual reporting is bound by errors, modern pathology departments today have automatic digital systems. Large lab networks process hundreds of cancer specimens every week, where digital systems are imperative. While they improve accuracy, they ensure turnaround times without delays.
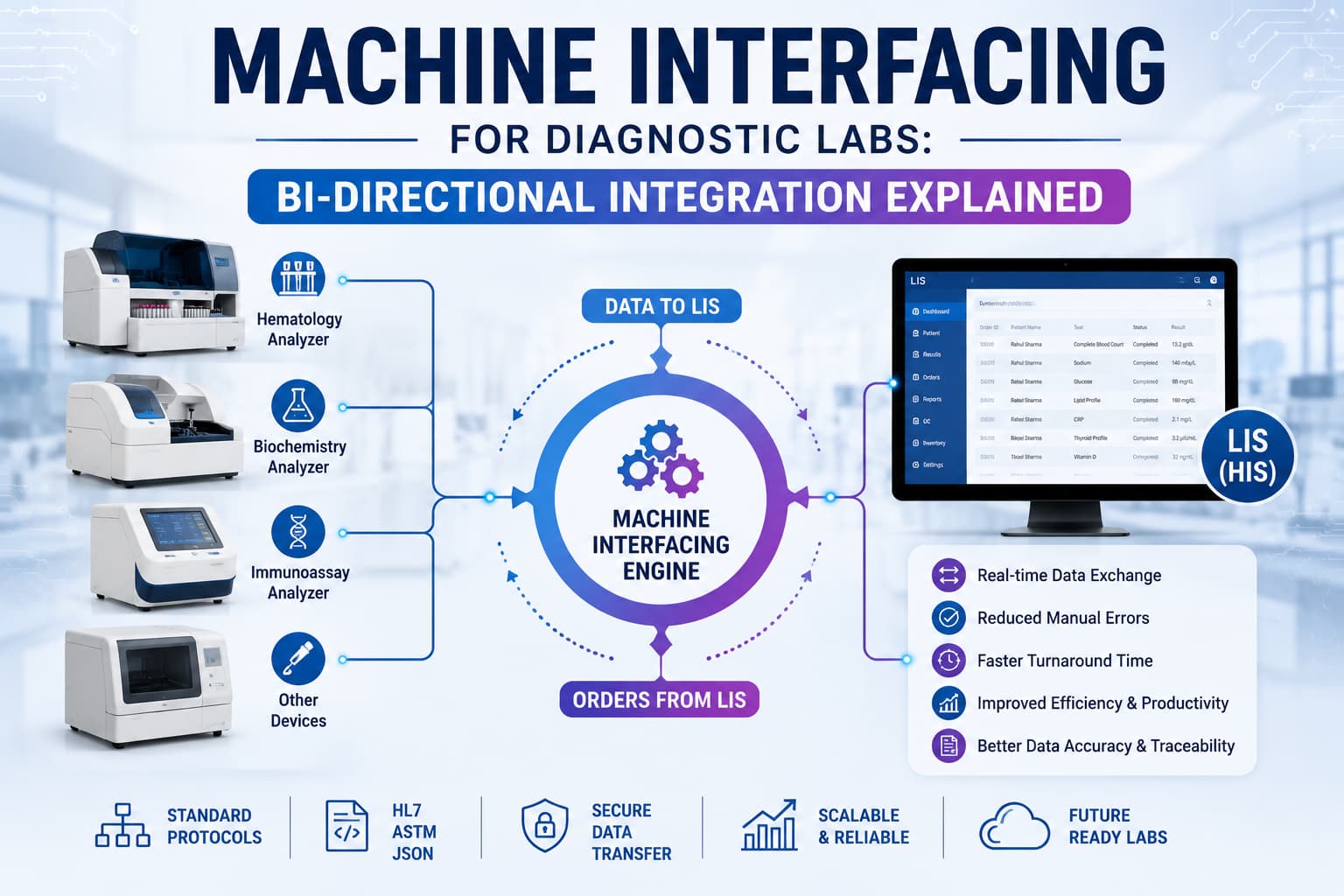
Among the lab automation, laboratory information systems are the most important. They bring order to diagnostic data in an unprecedented way.
With automation in place for repetitive tasks, such systems strengthen reliability in the reporting of cancer grading and staging.
How AI-Powered LIS Platforms Support Oncology Diagnostics
Pathology labs across the world have adopted digital systems, which have evolved fast. Those digital pathology tools now integrate artificial intelligence and automated reporting modules.
They have improved the productivity manifold that laboratories today experience smoother case tracking and more consistent documentation.
The AI-powered FLABS is one such platform in India. It is an LIS that introduces several capabilities.
- AI-driven reporting with automated summaries of interpretation.
- Voice-to-report conversion that turns dictation into structured reports.
- Smart report templates.
- Real-time Turnaround Time (TAT) management for specimens.
- Bulk report approval and download.
- Automated quality control checks.
- Financial automation for billing and payment management.
- Referral partner tracking system.
- Secure QR-coded digital reports for easy patient access.
- Barcode-based specimen tracking.
- Custom patient data fields.
- Multiple digital signatures for departmental verification.
- Personalised interpretations aligned with laboratory standards.
In environments handling large volumes of oncology cases, such systems strengthen consistency in cancer grading and staging records.
Final Thoughts
Cancer classification extends far beyond detecting malignant cells.
By combining tumour differentiation with anatomical spread, cancer grading and staging present a complete disease profile. From breast and prostate malignancies to kidney, bladder, lung, and oesophageal tumours, the principle is consistent.
For pathology professionals, accurate grading, structured reporting, and integrated laboratory systems ensure reliable diagnostic communication across oncology teams.
And in a field where every detail shapes critical decisions, precision in cancer grading and staging is indispensable. LIS platforms like FLABS enable that with advanced software.
Ready to Upgrade Your Lab Operations? Start Your 5-Day Free Trial Today with FLABS AI-Powered LIS
Get Started at ₹1!
Try Flabs for a full month for just ₹1.
Follow us on